1-(844)-420-ACIA (2242) Mon-Fri : 8:00 AM - 5:00 PM
This page is for tracking the ACIA’s progress towards applying with the Arkansas Department of Health (ADH) to add Irritable Bowel Syndrome (IBS) as a qualifying condition.
We have chosen IBS because of the condition’s similarity to Crohn’s Disease, which is already one of the qualifying conditions. In other words, it should be an easy one to add, and it will be a good test of the ADH’s willingness to add additional qualifying conditions.
Below is the petition form from the ADH and our information and notes gathered in preparation for submitting the petition.
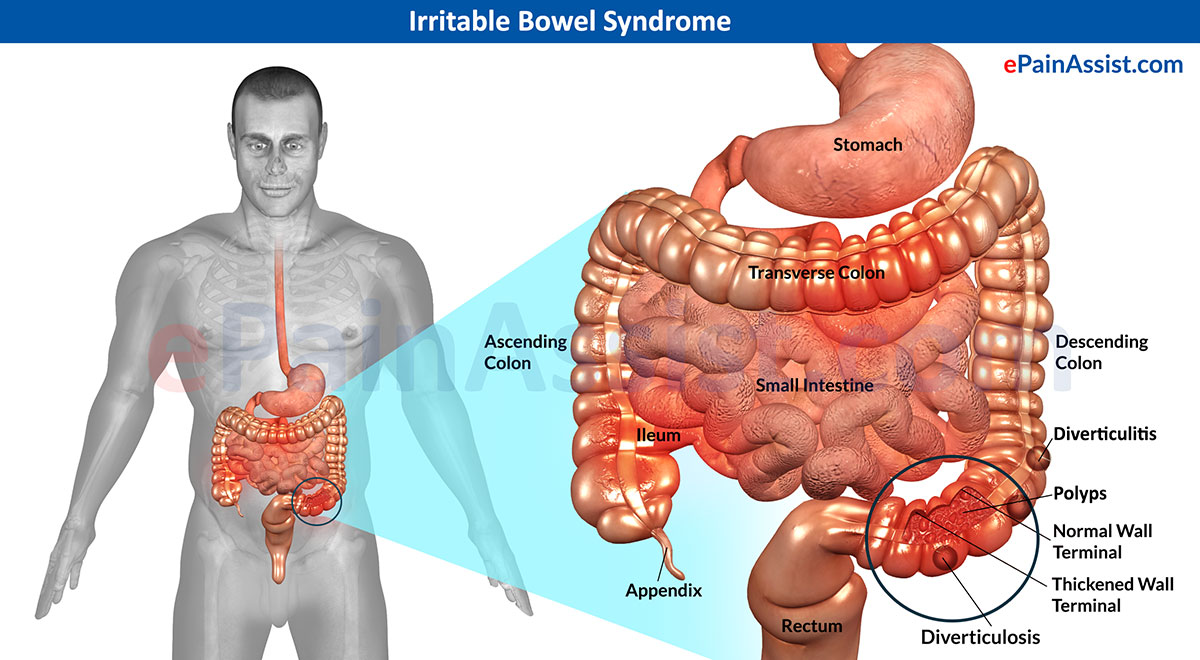
IBS is classified according to the primary symptoms displayed by each patient. Thus diarrhea, constipation, and alternating diarrhea with constipation and infection become the basis for diagnosing the disease as IBS-D, IBS-C, IBS-A, or post-infectious IBS-PI, respectively. Ulcerative colitis is a form of IBD that can affect other body parts as well. Crohn’s disease, another form of IBD, is an autoimmune disorder affecting the gastrointestinal tract.
Other frequently observed symptoms may include abdominal discomfort (gas, bloating, cramps), the sensation of incomplete void of stool, gastroesophageal reflux disease (GERD), anxiety, depression, pain (abdominal, back, head, muscle), increased generalized weakness, and lack of energy.
Case reports from cannabis-using IBS patients suggest that cannabis may be effective in managing some symptoms, especially nausea, diarrhea, stress, cramps, and lack of appetite.
Doctors may recommend patients try some of the following medicines to relieve IBS symptoms:
When taken over a protracted period, many of these drugs cause side effects. For example, abruptly stopping antidepressants can cause withdrawal symptoms. Side effects of antidepressants include:
Antidepressants can even make patients feel suicidal in the worst-case scenario. Both antidepressants and antispasmodics can worsen constipation. Muscle relaxants are prescribed in these cases. Unfortunately, muscle relaxants contain a mild sedative that can be habit forming. Even fiber supplements and laxatives can have adverse effects. Some people report worsened gas and bloating from supplements. Laxatives can be habit forming when used too often. Some people report nausea as a side effect of taking peppermint capsules.
Other conventional IBS treatments include:
Approximately 35 million Americans are impacted by IBS.
Research is being carried out in the field of medical marijuana for irritable bowel syndrome. Some evidence suggests that your body’s endocannabinoids, the molecules in your body that resemble compounds found in pot, could help limit intestinal inflammation. People with IBD have higher levels of cannabinoid receptors in their colon. There have been some small studies that show many patients take medical cannabis for irritable bowel syndrome symptoms.
Even though cannabis and irritable bowel syndrome research and treatment recommendations are still in their infancy, there are ways pot can improve your quality of life. Marijuana can ease three main symptoms of IBS — depression, diarrhea and abdominal pain.
IBS affects patients’ mental well-being. Cannabis is a well-known mood lifter. Just a little can make a patient feel far more positive. A study published in April 2016 in the journal Neuropharmacology discovered a non-psychoactive substance in cannabis, cannabidiol (CBD), eases anxiety and antisocial behaviors in rodents in minutes. The effects continued to work over time. Conventional antidepressants can take weeks to work. Cannabis could work wonders for you if you feel depressed as a result of your illness.
Diarrhea is a debilitating, painful and embarrassing symptom of IBS. Cannabis has been shown to help with diarrhea by reducing the rate food moves through your gastrointestinal tract while minimizing abdominal cramping.
A study published in the British Journal of Pharmacology suggests cannabinoid treatments can help manage diseases like IBS. Pot is both anti-inflammatory and works well at alleviating nerve pain. Another study points to cannabinoid treatments calming intestinal lining inflammation and sensitivity in people with GI problems.
Robert deBin: Can’t make today’s call but my dr Williams update is: I’ve been in touch with his assistant. Gave her all the info. Dr. Williams is out of town until next week. Hope to hear something then.
Conference call notes:
Conference Call notes:
Letter from Dr. Joe Goldstrich:
The use of cannabinoids in the management of Irritable Bowel Syndrome
Good afternoon to everyone!
Joe Goldstrich, MD, FACC
Dr. Joe is Board-Certified in Internal Medicine, Cardiology, and Clinical Lipidology, with a distinguished career in traditional medicine, nutrition, lipid management and preventive cardiology. He is a Fellow of the American College of Cardiology and the former National Director of Education and Community Programs for the American Heart Association. Since 2012, he has specialized in medical cannabis, helping patients utilize cannabis as part of their traditional medical treatment. He currently serves as a member of the Board of Directors for the Society of Cannabis Clinicians and holds an active California medical license.
Dustin Sulak, D.O.
Dr. Dustin Sulak is a renowned integrative medicine physician based in Maine. He has helped 18,000+ patients and is nationally regarded as an expert on medical cannabis. Dr. Sulak holds the distinction of being a Diplomat of the American Academy of Cannabinoid Medicine. He lectures on medical cannabis and the endocannabinoid system nationally. Dr. Sulak currently serves as a member of the Board of Directors for the Society of Cannabis Clinicians.
Dr. Russo,
Dr. Sulak,
Conference Call Notes:
From Baron Crane: I have reached out to Dr Dustin Sulak and am waiting for a reply. He is a medical cannabis doctor in Maine who has experience treating IBS patients. Maine is one of the few states that recognize IBS as a qualifying condition and Dr Sulak is the only doctor I have been able to find so far that discusses treating IBS. If we can find a doctor that has patient experience treating IBS with cannabis that is willing to write a testimony that could be the key to getting it approved.
From Bradley Phillips – Network of experts and advocates:
https://irritablebowelsyndrome.net/experts/
From Storm Nolan – I spoke with Joy Gray today, the head of the MMJ division at the ADH. She confirmed that they haven’t received an application yet to add a qualifying condition. Let’s be the first!
From Robbin Rahman – Here is our statutorily established evidentiary burden:
Section 4(c)(2) of the AMMA: “In considering a petition, the department shall add medical conditions or treatments to the list of qualifying conditions set forth in section 2 of this amendment if patients suffering medical conditions or undergoing the treatments in question would derive therapeutic benefit from the use of marijuana, taking into account the positive and negative health effects of such use.”
The DOH form requires us to make additional, different showings, but I think if they deny it and we decide to seek an appeal through a lawsuit, this is the burden that we have to make absolutely sure we carry.
So the first step in my mind is making sure we have gathered as much evidence as possible of a “therapeutic benefit.” I presume this has a clinical meaning – perhaps one of the doctors or Brandon could chime in on this.
The Arkansas Supreme Court just ruled that the legislature cannot waive sovereign immunity (the concept that you can’t sue the state). Very controversial and could mean that you can’t sue under AFOIA now, which is crazy.
Luckily, the appeal right for adding conditions is set forth in a Constitutional amendment, so we should still be able to appeal the decision of the DOH.
From Brandon Thornton: I think this Russo article is a good place to start. He makes a compelling case for using cannabis to treat IBS and includes strong references to back his points. Most of his references are paid-access articles, but I think I can access these from the UAMS Pharmacy School drug info center (I’m going to try anyway). We can follow his lead and build a case based on his references and any other peer-reviewed articles that have been published since. Let’s make it impossible for the BOH to say no!